9 March, 2017
It's Friday night, 23 May 2014. Sydney is experiencing its warmest May on record and its second of four consecutive warm days. One of Sydney's flagship festivals, Vivid Sydney (an annual winter outdoor lighting festival) is taking place. During the three week festival, more than 1.43 million people will attend.
The evidence before this inquest left a distinct impression of uncertainty as to the procedures to be followed and by whom in the event of an emergency of this nature…there were a number of systems failures relevant to the manner of Mr Hickey's death.
A group of friends meet at a bar in Martin Place. They decide to attend Vivid Darling Harbour to watch the light and sound show. On route, they purchase some snacks and bottles of wine and take position around 9pm at the waters' edge on the eastern promenade just south of the entry to the Cockle Bay Marina.
The group is approached about half an hour later, by the coxswain of Seahawk II, a Sydney Harbour Foreshore Authority (SHFA) vessel. The coxswain informs the group that it is an offence to consume alcohol in Darling Harbour and advises the group to cease drinking in the area. One of the group members apologises and they move to another area. The group repositions themselves on the eastern boardwalk about 20 metres south of the entrance of the marina, adjacent to the water's edge, not far from Home Nightclub.
Just before 11pm, the group decides to leave the area and go to dinner. A member of the group, Mr Brendan Hickey starts to stand up, loses his balance and falls into the water. Mr Hickey, being unable to swim, sinks under the water and dies.
Fast -forward to 22 December 2016 and Deputy State Coroner Magistrate Teresa O'Sullivan hands down her findings and recommendations in the Inquest into the Death of Brendan Hickey. The inquest subsequently finds that Mr Hickey died as a consequence of drowning by misadventure to which alcohol intoxication was a contributing factor.
Coroner's Findings
The findings and recommendations are worth exploring as they move beyond the direct cause and nature of Mr Hickey's death. The Deputy State Coroner went so far as to examine the systems implemented by both public and private sector organisations involved in the event's management stating that:
"the evidence before this inquest left a distinct impression of uncertainty as to the procedures to be followed and by whom in the event of an emergency of this nature…there were a number of systems failures relevant to the manner of Mr Hickey's death" (at para 59).
As a result, there are a series of lessons for event, contractor and risk management arising from the Deputy State Coroner's analysis.
Here are five of those lessons:
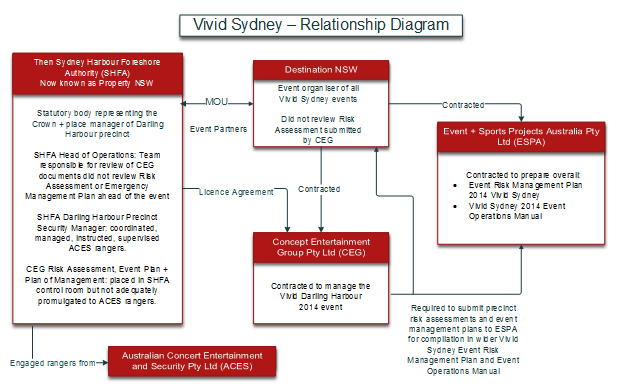
1. Develop co-ordination plans: communicate and co-ordinate your activities with all involved in the event – The management of Vivid involved a number of different entities. NSW public sector agencies Destination NSW and what was then known as SHFA (now Property NSW) engaged a number of contractors and subcontractors for various aspects of the management of Vivid 2014. Here is a basic diagram outlining the entities and contractual relationships:
Please click on the image to enlarge.
Through the variety of Event Plans, Event Management Plans, Site Safety Plans, Emergency Plans, Risk Assessments and procedures prepared by the organisations, there were numerous inconsistencies described and gaps in understanding of the roles and responsibilities between the parties, particularly in emergency management. Indeed, under CEG's emergency management plan, the actions required of staff in the event of an incident were inconsistent with the chain of command. These issues also led to failings in monitoring and supervising the risk assessment work of contractors in planning for the event.
When you have many different organisations involved in achieving an outcome (such as planning and managing a major event like Vivid), it is crucial for plans to be developed that articulate how the organisations will consult, co-operate and co-ordinate with each other in relation to health and safety matters. Indeed, this is a legal obligation set out in section 46 of the Work Health and Safety Act 2011 (NSW).
2. Select the right contractors in the first place – review their approach to safety risk management as part of the selection process – As we often advise our clients, if you select the right contractor, the rest tends to fall into place. The evidence in the inquest identified that the precinct risk assessments submitted by contractors were significantly deficient. Identifying and assessing the safety management skills, qualifications and experience of project team personnel for core requirements (including safety management) should be part of the contractor selection process.
3. Train people in effective hazard and risk management – The Deputy State Coroner heard evidence that: "even a cursory examination of the CEG Risk Assessment applying the risk management principles and a critical mind would disclose that [the risk assessment] is entirely inadequate". The risk assessment did not identify the risk to members of the public presented by the open waters' edge of Cockle Bay and as a result, did not assess the need for controls to manage that risk. SHFA had a number of controls in place at the time of the incident (such as lifebuoys; fixed emergency ladders; some signage; ranger patrol services; patrol boats; and some CCTV monitoring) but their adequacy specifically in light of the event was not considered because of the failure to identify the risk in the context of planning for Vivid Darling Harbour. For instance, identifying the risk may have led to consideration of temporary barriers to isolate the open waters' edge during the event.
The inquest heard that the CEG risk assessment had been prepared by an employee who had no skills, qualifications or expertise in risk management nor had he attended any risk assessment training. The content of the CEG Vivid Darling Harbour risk assessment was based on previous risk assessment documents he had seen 'over many years'. Workers need applied skills training in hazard and risk management (including the process and steps required by health and safety laws).
4. Cross-check: contracting out does not absolve you from monitoring contractors' approach to planning and operations – CEG had submitted its risk assessment to Destination NSW as well as overall event management company ESPA. While the contract with ESPA required precinct risk assessments to be submitted to ESPA for compilation into the whole-of-event plans, neither Destination NSW nor ESPA provided feedback on the adequacy of the risk assessments submitted by CEG. The contract between Destination NSW and ESPA did not require ESPA to conduct any cross-checking of site specific risk assessments to ensure consistency across all plans submitted by the various contractors engaged for different programs in the wider event. In essence, it appears ESPA fulfilled a compilation role rather than one of co-ordination.
The Deputy State Coroner found that: "the failure to have in place a system of cross-checking, designed to ensure consistency of approach to risk management and planning across the event – including adherence to relevant standards and best industry best practice – represents a significant omission in the context of overlapping and inter-related safety management systems under which the event was being produced." (see para 72).
It is critical to have well implemented systems for monitoring safety performance in practice throughout the life of a contract: from planning through to operations and handover.
5. Conduct co-ordinated emergency scenario training and testing with those that need to implement emergency procedures including all relevant stakeholders – The CEG Vivid Event Manager did not have training in, nor consult, CEG's Vivid 2014 Show Stop Procedure in making decisions as to whether the Vivid Aquatique water show event should continue following the incident. Authorising the light and sound show to continue also meant that police rescue officers unknowingly entered water containing high voltage cables.
While the evidence indicated it was unlikely that the electrical installation presented an immediate risk to those in the water because the joins were all above ground, the additional precautionary measure of isolating the electrical installation did not occur until about 11.40pm, approximately 20 minutes after a police rescue worker had entered the water. The show's sound component also hampered police rescue efforts to co-ordinate an effective response.
Further, the other organisations involved in the event's management (such as Destination NSW, SHFA and ACES) did not appear to be aware of the Show Stop Procedure. Neither the Darling Harbour Precinct Manager nor the Ranger Supervisor from SHFA was aware of this procedure. The Deputy State Coroner took the view that the appropriate approach would have been to postpone commencement of the show and await police arrival at the scene for their advice as to whether the show should go ahead.
Clear roles, responsibilities and processes need to be outlined in single shared emergency management plans and procedures. Their adequacy then needs to be tested in scenarios that involve all those who would play a role in their implementation in the event of incident.
Please click on the image to enlarge.

Coroner's Recommendations
The Deputy State Coroner made recommendations for CEG directors to "give urgent consideration" to:
- retaining a qualified risk management consultant to perform a review of the company's risk management policies, practices and procedures; and
- engaging qualified risk management consultants to provide formal documented training to directors, officers and employees who are required to conduct risk assessments and prepare event management and emergency management plans.
The Deputy State Coroner also made recommendations for the minister responsible for Property NSW and the CEO of Place Management NSW including that they "give urgent consideration" to:
- establishing an independent review of the risk assessment and risk management systems of Place Management NSW for planning and conduct of events held on Place Management land (including events organised by third parties);
- developing documented identified quantifiable criteria for defining "major" or "large scale" events to be held in the Darling Harbour precinct at which the event manager must be required to erect temporary barriers to isolate the open waters' edge of Cockle Bay for public safety purposes; and
- establishing a systematic review of the corporate "Risk Decision Criteria" used by Place Management NSW, in assessing risks to public safety associated with the open waters' edge at Cockle Bay wharf with the purpose of the review being to ensure there is an appropriate balance struck between the design objectives associated with the preservation of an open waters; edge to Cockle Bay and the need to ensure public safety in the ongoing management of the Darling Harbour precinct.
![]()
For further information, please contact:
Alena Tittert, Partner, Clyde & Co
alena.tittert@clydeco.com


